Covid19mathblog.com
Amazing chart below to think about – now with 3 years of data.
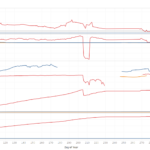
First set shows the 7 day average confirmation cases. This gives the indication of how rapidly the virus is spreading.
The second charts shows the 7 day average deaths.
The 3rd chart shows the 30 day moving average of deaths/confirmation. This is trying to show the fatality rate giving an indication of how well our medical treatment and/or vaccine effectiveness to reduce fatalities.
The fourth chart shows the fully vaccinated over the population – vaccination rate 18+
The fifth chart is the annual running tally of deaths each year.

Important to see we have been over 60% vaccinated this year whereas last year this time less than 7%. Yet we have way more confirmation – hence the vaccine did not stop transmission – even just a little bit – and even though those were the promises made in the beginning – https://www.realclearpolitics.com/video/2021/10/07/biden_vaccinated_protected_from_covid_cannot_spread_it_to_you.html
The politicizing of covid would eventually catch up as the ability of govt to actually control and limit an unknown in a discrete time period is nearly impossible without some nature luck – deaths in the US last year was way above the bar of 220K as stated – this certainly did not age well – https://twitter.com/JoeBiden/status/1319446692236791814?t=gChxktazKr1lyWUzrJLrqw&s=19

One of the best graphics on covid was developed in Canada. They realize reporting totals without age, health, and vaccination amount can skew the view and create unnecessary fear. https://news.gov.bc.ca/files/1.21.22_COVID_Hospitalizations.pdf
Stay healthy and the odds will be in your favor – as you get older 50+ vaccination is advised even when healthy. This is the message that should have been told in the beginning.

An interesting piece which perhaps causes some vaccination hesitancy but perhaps valid. As noted the bioaccumulation aspect of spike protein would be concerning on a long time line. Elderly less risk of this being an issue. Data from Pfizer and Moderna could be used to alleviate some of these concerns but this data is still limited. https://covidmythbuster.substack.com/p/what-happens-to-those-billions-of?utm_source=url
“The number of nanoparticles (NP) injected in a dose of these anti-COVID vaccines is utterly flabbergasting: up to 50 billion viral vectors for AstraZeneca, 40 billion LNPs for Moderna, and likely 10 for Pfizer. It’s not very clear how many intact messenger RNA are in each LNP , but even if we agree to only 1, and that each one produces 1000 spike protein, we are talking your body having to deal with a minimum 30 trillion pathogenic spike proteins2 in a few months time…
Those are numbers way beyond very severe SARS-COV-2 infections: typically at infection peak between 1 and 100 billion virions, are present in the body.
What the medical and public health community hasn’t realised is that all the healthy cells that will be “infected”3 by these nanoparticles will eventually be destroyed by the immune system. When you take the Pfizer vaccine 3 times, you accept sacrificing up to 45 billion of your healthy cells… with AstraZeneca it’s 150 billion!”
Public message to get well and healthy is becoming more and more important with over 23% of the population confirmed with covid. Those recovered from covid hold some long term heart issues (also noted with vaccination) – https://www.nature.com/articles/s41591-022-01689-3
“Our results provide evidence that the risk and 1-year burden of cardiovascular disease in survivors of acute COVID-19 are substantial. Care pathways of those surviving the acute episode of COVID-19 should include attention to cardiovascular health and disease.”
Exercise is important – you cannot pill/vaccinate your way to health as demonstrated – https://www.science.org/doi/10.1126/sciadv.abl4988
“we demonstrate that skeletal muscle NADPH oxidase 4 (NOX4), which is induced after exercise, facilitates ROS-mediated adaptive responses that promote muscle function, maintain redox balance, and prevent the development of insulin resistance. Conversely, reductions in skeletal muscle NOX4 in aging and obesity contribute to the development of insulin resistance. NOX4 deletion in skeletal muscle compromised exercise capacity and antioxidant defense and promoted oxidative stress and insulin resistance in aging and obesity. The abrogated adaptive mechanisms, oxidative stress, and insulin resistance could be corrected by deleting the H2O2-detoxifying enzyme GPX-1 or by treating mice with an agonist of NFE2L2, the master regulator of antioxidant defense. These findings causally link NOX4-derived ROS in skeletal muscle with adaptive responses that promote muscle function and insulin sensitivity.”
So here I will present some conflicting paper – first we start with paper declaring vaccine is superior over natural immunity and note the funding sources – https://www.medrxiv.org/content/10.1101/2022.02.10.22270789v1
“while Omicron-based immunogens may be adequate boosters, they are unlikely to be superior to existing vaccines for priming in SARS-CoV-2 naïve individuals.”
“Funding Statement
PLM is supported by the South African Research Chairs Initiative of the Department of Science and Innovation and National Research Foundation of South Africa, the SA Medical Research Council SHIP program, the Centre for the AIDS Programme of Research in South Africa (CAPRISA). We acknowledge funding from the Bill and Melinda Gates Foundation, through the Global Immunology and Immune Sequencing for Epidemic Response (GIISER) program. SIR is a LOreal/UNESCO Women in Science South Africa Young Talents awardee.”
Now papers supporting natural immunity superior – https://jamanetwork.com/journals/jama/fullarticle/2788894
“Although evidence of natural immunity in unvaccinated healthy US adults up to 20 months after confirmed COVID-19 infection is encouraging, it is unclear how these antibody levels correlate with protection against future SARS-CoV-2 infections, particularly with emerging variants. The public health implications and long-term understanding of these findings merit further consideration.”
“Funding/Support: This work was supported by charitable donations from the Ben-Dov family.
Role of the Funder/Sponsor: The Ben-Dov family had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data, preparation, review, or approval of the manuscript, and decision to submit the manuscript for publication.”
https://www.nejm.org/doi/full/10.1056/NEJMc2200133
“Overall, in a national database study in Qatar, we found that the effectiveness of previous infection in preventing reinfection with the alpha, beta, and delta variants of SARS-CoV-2 was robust (at approximately 90%), findings that confirmed earlier estimates.1-3 Such protection against reinfection with the omicron variant was lower (approximately 60%) but still considerable. In addition, the protection of previous infection against hospitalization or death caused by reinfection appeared to be robust, regardless of variant.”
“Supported by the Biomedical Research Program and the Biostatistics, Epidemiology, and Biomathematics Research Core at Weill Cornell Medicine–Qatar; the Qatar Ministry of Public Health; Hamad Medical Corporation; and Sidra Medicine. The Qatar Genome Program and Qatar University Biomedical Research Center supported viral genome sequencing.”
Given the above which view would you take for natural immunity?
Now we have data censorship because we cant interpret data and/or cant handle the truth? https://www.dailymail.co.uk/news/article-10537161/CDC-refusing-publish-data-collected-booster-effectiveness-aged-18-49.html
“CDC is refusing to publish data it has collected on booster effectiveness for 33 MILLION Americans aged 18-49 over fears it might show the vaccines as ineffective: FDA expert tells CDC to ‘tell the truth’
Two weeks ago the Centers for Disease Control and Prevention (CDC) published data about the effectiveness of boosters against COVID-19
The CDC failed to publish a tranche of their data, however – omitting the impact on those aged 18-49, who are least likely to benefit from boosters
The CDC are also being criticized for failing to publish their information about child hospitalization rates and comorbidities
A spokeswoman for the CDC said they were concerned that the data would be misinterpreted, pointing out that it was incomplete and not verified
Critics said that it was always better to publish the information rather than withhold, and allow scientists to analyze and explain what they could”
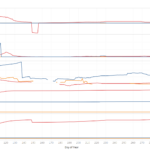
The US is finally not the top confirmation country – still tops on death.

Iceland over 80% vaccinated but they are soaring in confirmations – deaths are also approaching the highs in 2020.

TX leading confirmations and deaths now – followed by CA.

TX death is in the population centers.

Relative to last year a large spike in confirmation – but deaths have been in the same region until recently

Similar picture in CA – large spike but rapid drop in confirmation.

Similar in NY – rapid fall in confirmation

Added NY and FL to the graph. NY generally masked – FL not. What is interesting to see is Miami/Dade and Queens have one of the highest vaccination rate among all the major counties/cities yet also observe very high transmission rates.