Covid19mathblog.com
As noted early on here there was something going on with vaccines and the female reproductive system – perhaps it will turn out completely harmless but still know one knew for sure. Now the NIH will put some money behind it to close the issue – https://nypost.com/2021/09/07/nih-to-study-how-covid-19-vaccine-impacts-menstrual-cycle/amp/
“The National Institutes of Health has announced a $1.67 million study to investigate reports that suggest the COVID-19 vaccine may come with an unexpected impact on reproductive health.
It’s been a little over six months since the three COVID-19 vaccines in the US — Pfizer, Moderna and Johnson & Johnson — became widely available to all adults. But even in the early days of vaccine rollout, some women were noticing irregular periods following their shots, as reported first by the Lily in April.”
“It would appear that the NIH heard Clauson and others’ reports, as they announced on Aug. 30 that they intended to embark on just such research — aiming to incorporate up to half a million participants, including teens and transgender and nonbinary people.
Researchers at Boston University, Harvard Medical School, Johns Hopkins University, Michigan State University and Oregon Health and Science University have been enlisted to embark on the study, commissioned by the NIH’s National Institute of Child Health and Human Development (NICHD) and the Office of Research on Women’s Health.”
“The approximately yearlong study will follow initially unvaccinated participants to observe changes that occur following each dose. More specifically, some groups will exclude participants on birth control or gender-affirming hormones, which may have their own impact on periods.
“Our goal is to provide menstruating people with information, mainly as to what to expect, because I think that was the biggest issue: Nobody expected it to affect the menstrual system, because the information wasn’t being collected in the early vaccine studies,” said NICHD director Diana Bianchi in a statement to the Lily — reportedly crediting their early coverage for helping to make the NIH aware. The NIH suggests that changes to the menstrual cycle could arise out of several of life’s circumstances during a pandemic — the stress of lifestyle changes or possibly contending with illness. Moreover, the immune and reproductive systems are intrinsically linked, and the notion that the immune-boosting vaccine may disrupt the typical menstrual cycle is plausible, as demonstrated by previous studies concerning vaccine uptake. “
“It’s also worth noting the vaccine does not cause infertility and the Centers for Disease Control and Prevention recommends the shot even for pregnant women.
As changes to the menstrual cycle are “really not a life and death issue,” explained Bianchi, the Food and Drug Administration — fast-tracking their work — prioritized only the most critical risks associated with the COVID-19 vaccine.
The NIH, too, pulled together the initiative at breakneck speed. Funding for such a study would typically take years to see approval.
“We were worried this was contributing to vaccine hesitancy in reproductive-age women,” said Bianchi.”
For clarification when the CDC states the above “It’s also worth noting the vaccine does not cause infertility and the Centers for Disease Control and Prevention recommends the shot even for pregnant women.” it doesn’t mean its not possible it’s just they don’t have any evidence yet per own website: “Currently no evidence shows that any vaccines, including COVID-19 vaccines, cause fertility problems (problems trying to get pregnant) in women or men.”
There is not a one size fits all for health decisions. Each person has their own risk/reward – as long as we are all educated and not coerced we can make the best decisions. And this includes understanding the impact on others from your decision.
Finally some traction on ventilation – I don’t think the cost are as much as noted in the paper – simple adjustments to economizers in commercial buildings can be done now. We just need a targeted benchmark of ventilation – I propose the same level Taiwan focuses on 1000ppm CO2. Creating buildings that breath will likely increase our power consumption but in the grand scheme of things that cost is miniscule compared to the health benefits https://www.theatlantic.com/health/archive/2021/09/coronavirus-pandemic-ventilation-rethinking-air/620000/?utm_source=feed
“To understand why pathogens can spread through the air, it helps to understand just how much of it we breathe. “About eight to 10 liters a minute,” says Catherine Noakes, who studies indoor air quality at the University of Leeds, in England. Think four or five big soda bottles per minute, multiply that by the number of people in a room, and you can see how we are constantly breathing in one another’s lung secretions.”
“Even before SARS-CoV-2, studies of respiratory viruses like the flu and RSV have noted the potential for spread through fine aerosols. The tiny liquid particles seem to carry the most virus, possibly because they come from deepest in the respiratory tract. They remain suspended longest in the air because of their size. And they can travel deeper into other people’s lungs when breathed in; studies have found that a smaller amount of influenza virus is needed to infect people when inhaled as aerosols rather than sprayed up the nose as droplets. Real-world evidence stretching back decades also has suggested that influenza could spread through the air. In 1977, a single ill passenger transmitted the flu to 72 percent of the people on an Alaska Airlines flight. The plane had been grounded for three hours for repairs and the air-recirculation system had been turned off, so everyone was forced to breathe the same air.”
“In official public-health guidance, however, the possibility of flu-laden aerosols still barely gets a mention. The CDC and World Health Organization guidelines focus on large droplets that supposedly do not travel beyond six feet or one meter, respectively. (Never mind that scientists who actually study aerosols knew this six-foot rule violated the laws of physics.) The coronavirus should get us to take the airborne spread of flu and colds more seriously too, says Jonathan Samet, a pulmonary physician and epidemiologist at the Colorado School of Public Health. At the very least, it should spur research to establish the relative importance of different routes of transmission. “We had done such limited research before on airborne transmission of common infections,” Samet told me. This just wasn’t seen as a major problem until now.”
“A virus that lingers in the air is an uncomfortable and inconvenient revelation. Scientists who had pushed the WHO to recognize airborne transmission of COVID-19 last year told me they were baffled by the resistance they encountered, but they could see why their ideas were unwelcome. In those early days when masks were scarce, admitting that a virus was airborne meant admitting that our antivirus measures were not very effective. “We want to feel we’re in control. If something is transmitted through your contaminated hands touching your face, you control that,” Noakes said. “But if something’s transmitted through breathing the same air, that is very, very hard for an individual to manage.”
The WHO took until July 2020 to acknowledge that the coronavirus could spread through aerosols in the air. Even now, Morawska says, many public-health guidelines are stuck in a pre-airborne world. Where she lives in Australia, people are wearing face masks to walk down the street and then taking them off as soon as they sit down at restaurants, which are operating at full capacity. It’s like some kind of medieval ritual, she says, with no regard for how the virus actually spreads. In the restaurants, “there’s no ventilation,” she adds, which she knows because she’s the type of scientist who takes an air-quality meter to the restaurant.”
“If buildings are allowing respiratory viruses to spread by air, we should be able to redesign buildings to prevent that. We just have to reimagine how air flows through all the places we work, learn, play, and breathe.”
“The pandemic has already prompted, in some schools and workplaces, ad hoc fixes for indoor air: portable HEPA filters, disinfecting UV lights, and even just open windows. But these quick fixes amount to a “Band-Aid” in poorly designed or functioning buildings, says William Bahnfleth, an architectural engineer at Penn State University who is also a co-author of the Science editorial. (Tellier, Noakes, and Milton are authors too; the author list is a real who’s who of the field.) Modern buildings have sophisticated ventilation systems to keep their temperatures comfortable and their smells pleasant—why not use these systems to keep indoor air free of viruses too?
Indeed, hospitals and laboratories already have HVAC systems designed to minimize the spread of pathogens. No one I spoke with thought an average school or office building has to be as tightly controlled as a biocontainment facility, but if not, then we need a new and different set of minimum standards. A rule of thumb, Noakes suggested, is at least four to six complete air changes an hour in a room, depending on its size and occupancy. But we also need more detailed studies to understand how specific ventilation levels and strategies will actually reduce disease transmission among people. This research can then guide new indoor air-quality standards from the American Society of Heating, Refrigerating and Air-Conditioning Engineers (ASHRAE), which are commonly the basis of local building codes. Changing the building codes, Bahnfleth said, is what will actually get buildings to change their ventilation systems.”
“The challenge ahead is cost. Piping more outdoor air into a building or adding air filters both require more energy and money to run the HVAC system. (Outdoor air needs to be cooled, heated, humidified, or dehumidified based on the system; adding filters is less energy intensive but it could still require more powerful fans to push the air through.) For decades, engineers have focused on making buildings more energy efficient, and it’s “hard to find a lot of professionals who are really pushing indoor air quality,” Bahnfleth said. He has been helping set COVID-19 ventilation guidelines as chair of the ASHRAE Epidemic Task Force. The pushback based on energy usage, he said, was immediate. In addition to energy costs, retrofitting existing buildings might require significant modifications. For example, if you add air filters but your fans aren’t powerful enough, you’re on the hook for replacing the fans too.”
Lets not forget to learn about the source of this catastrophic event so we wont repeat this! – https://theintercept.com/2021/09/06/new-details-emerge-about-coronavirus-research-at-chinese-lab/
“NEWLY RELEASED DOCUMENTS provide details of U.S.-funded research on several types of coronaviruses at the Wuhan Institute of Virology in China. The Intercept has obtained more than 900 pages of documents detailing the work of EcoHealth Alliance, a U.S.-based health organization that used federal money to fund bat coronavirus research at the Chinese laboratory. The trove of documents includes two previously unpublished grant proposals that were funded by the National Institute of Allergy and Infectious Diseases, as well as project updates relating to EcoHealth Alliance’s research, which has been scrutinized amid increased interest in the origins of the pandemic.”
““This is a road map to the high-risk research that could have led to the current pandemic,” said Gary Ruskin, executive director of U.S. Right To Know, a group that has been investigating the origins of Covid-19.
One of the grants, titled “Understanding the Risk of Bat Coronavirus Emergence,” outlines an ambitious effort led by EcoHealth Alliance President Peter Daszak to screen thousands of bat samples for novel coronaviruses. The research also involved screening people who work with live animals. The documents contain several critical details about the research in Wuhan, including the fact that key experimental work with humanized mice was conducted at a biosafety level 3 lab at Wuhan University Center for Animal Experiment — and not at the Wuhan Institute of Virology, as was previously assumed. The documents raise additional questions about the theory that the pandemic may have begun in a lab accident, an idea that Daszak has aggressively dismissed.”
“The bat coronavirus grant provided EcoHealth Alliance with a total of $3.1 million, including $599,000 that the Wuhan Institute of Virology used in part to identify and alter bat coronaviruses likely to infect humans. Even before the pandemic, many scientists were concerned about the potential dangers associated with such experiments. The grant proposal acknowledges some of those dangers: “Fieldwork involves the highest risk of exposure to SARS or other CoVs, while working in caves with high bat density overhead and the potential for fecal dust to be inhaled.””
“Ebright also said the documents make it clear that two different types of novel coronaviruses were able to infect humanized mice. “While they were working on SARS-related coronavirus, they were carrying out a parallel project at the same time on MERS-related coronavirus,” Ebright said, referring to the virus that causes Middle East Respiratory Syndrome.”
“Biden blamed China for failing to release critical data, but the U.S. government has also been slow to release information. The Intercept initially requested the proposals in September 2020.
“I wish that this document had been released in early 2020,” said Chan, who has called for an investigation of the lab-leak origin theory. “It would have changed things massively, just to have all of the information in one place, immediately transparent, in a credible document that was submitted by EcoHealth Alliance.”
The second grant, “Understanding Risk of Zoonotic Virus Emergence in Emerging Infectious Disease Hotspots of Southeast Asia,” was awarded in August 2020 and extends through 2025. The proposal, written in 2019, often seems prescient, focusing on scaling up and deploying resources in Asia in case of an outbreak of an “emergent infectious disease” and referring to Asia as “this hottest of the EID hotspots.””
Noted before – variant identification requires genome sequencing – not only sparse but you cant even know what variant you have as not many labs are approved – https://www.businessinsider.com/covid-patients-cant-know-which-variant-infected-them-delta-2021-8
“The Centers for Medicare and Medicaid Service (CMS), which oversees the regulatory process for US labs, requires genome-sequencing tests to be federally approved before their results can be disclosed to doctors or patients. These are the tests that pick up on variants, but right now, there’s little incentive for the labs to do the work to validate those tests.
"I don’t think there’s a lot of motivation, quite honestly, to get that done," Kelly Wroblewski, director of infectious diseases at the Association of Public Health Laboratories, told Insider.”
“In some cases, knowing which variant is involved in an infection could inform how patients do their own contact tracing, since it informs how likely they are to have spread the virus others. (If it’s a Delta infection, for instance, they may want to notify a much wider circle of family and friends.)”
Talk about breaking the bonds of trust – this thread shows the amazing speed and desire to spread fake news as long as it fits the agenda –- https://twitter.com/DrewHolden360/status/1434591443855753220?t=YzZla71rgS9g8nbRs-7E5g&s=19
yes IVM has not proven to be the cure all conclusively but it’s a good risk/reward similar to why people take extra vitamin C.
Can you find some bad things on IVM – sure – here is a sterility issue with males but the study is lacking on many parts doesn’t account for recovery after not taking drug – study on rats – plus for me this is not a risky side of my equation – https://onlinelibrary.wiley.com/doi/abs/10.1111/and.12891
“We concluded that ivermectin has undesirable effects on male fertility and altered expression of IGFBP-3 and HSPA1 genes in the testes, while the administration of alpha lipoic acid can ameliorate the adverse effects of ivermectin”
Interesting to note the change in vaccine/vaccination definition on CDC

This change one could argue being healthy produces protection….so can we say a preparation of eating healthy and exercising daily is being vaccine and followed through that plan – you are then being vaccinated?
The youth surge in covid cases hard to get much concrete data on that. I did speak with a pediatric nurse and they are seeing it – but noted it is coming in tangent with RSV. Therefore to think Covid/Delta is independent that is not confirmed. We do know that quarantine kids for a year and kept in a super clean environment is not good for their immune system. IF you just allowed your kid to cruise the internet and eat process foods without much exercise that is also not good for the immune system (noted in previous blog – (Changes in Body Mass Index Among Children and Adolescents During the COVID-19 Pandemic | Adolescent Medicine | JAMA | JAMA Network) Also very likely catching RSV likely not helping the immune system to fight of Covid. All the above makes it hard to really point out it’s an opening school issue – yes directly if you kept your kid out of school forever perhaps will never get physically sick – we can’t protect them forever. Still the death rate numbers for youth is extremely low – well below car fatalities.
Collateral damage of policies to prevent Covid illness are real – https://www.medrxiv.org/content/10.1101/2021.02.13.21251670v6.full.pdf
“Countermeasures against COVID-19 outbreak such as lockdown and
voluntary restrictions against going out adversely affect human stress and economic
activity. Particularly, this stress might lead to suicide.”
“Conclusion:Excess mortality during the four months was more than two
times greater than the number of COVID-19 deaths confirmed by PCR testing.
Countermeasures against COVID-19 should be chosen carefully in light of suicide
effects.”
So we are a few months out before the official flu/cold season – the message is get your shots…I prefer the message to also focus on your health and build your immunity! – https://www.nbcnews.com/health/health-news/flu-season-coming-fast-miserable-studies-warn-rcna1909
Vaccination per capita for each country is interesting to view because in theory you don’t vaccinated under 12? It would seem Malta must be very old demographic or they went ahead and vaccinated the youth.

Vaccination campaign has resulted in an increase in vaccination in the US.

The US continues to be the leader in deaths and confirmation for covid – 652K deaths and climbing.

The same cohort states driving the summer numbers FL, TX, and CA

As compared to last year it’s the confirmations that are much higher – deaths are still lower driving the fatality rates really low – I am sure vaccines help drive this number down along with more awareness and treatment options.

Still county data doesn’t show the uvaxx vs vaxx is the driver of transmission

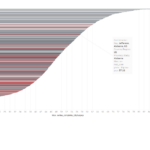
If we just look at one state – VT – a relatively high vaccinated states 62%– but still several counties with lower vaccination areas e.g. Franklin,Essex, and Caledonia (under 40%) – yet the second highest vaccinated county has the highest recent 7 day confirmation rate per capita.

In fact when we just look at Vermont compared to last year (below) this is one of the states that actually did not improve their fatality rates. More confirmation and more deaths than last year this time. Vaccine efficacy at least towards Delta (assuming delta) has to be questioned. If all we knew was VT.