Covid19mathblog.com
Data investigation to produce a forecast of covid deaths for this winter. First we need to understand the basic of the coronavirus which was noted back April 26th 2020 – Covid 4/26/20 | COVID 19 Information Page (covid19mathblog.com)
“One thing to unfortunately support the next wave is coming – is the understanding that weather does have a physical impact on the virus. As many of you know already the Covid virus is an envelope virus – meaning it has an outer shell covering the RNA. This shell adapts due to weather. It is very well described in this report – https://www.sciencedaily.com/releases/2008/03/080330203401.htm
““Like an M&M in your mouth, the protective covering melts when it enters the respiratory tract,” Dr. Zimmerberg said. “It’s only in this liquid phase that the virus is capable of entering a cell to infect it.”
In spring and summer, however, the temperatures are too high to allow the viral membrane to enter its gel state. Dr. Zimmerberg said that at these temperatures, the individual flu viruses would dry out and weaken, and this would help to account for the ending of flu season.
The finding opens up new possibilities for research, Dr. Zimmerberg said. Strategies to disrupt the virus and prevent it from spreading could involve seeking ways to disrupt the virus’s lipid membrane.
In cold temperatures, the hard lipid shell can be resistant to certain detergents, so one strategy could involve testing for more effective detergents and hand-washing protocols to hinder the spread of the virus.
Similarly, Dr. Zimmerberg added that flu researchers might wish to study whether, in areas affected by a severe form of the flu, people might better protect themselves against getting sick by remaining indoors at warmer temperatures than usual.”
Last statement certainly is true – the behavior in winter likely more inside less sun more central air recirculation etc….- but the physical change of the virus is a real phenomenon and makes sense in terms of evolutionary survival.”
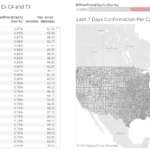
My hypothesis is HVAC temps likely cold enough to cause this encapsulation which plays a part in the summer spikes. Look at the last 4 weeks per capita confirmation most are in the warm states.

Knowing the physics we will see much higher confirmations in the winter as ALL states see cold enough environments that the virus will encapsulate.
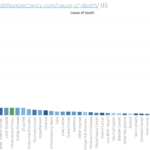
The chart below certainly shows vaccines have helped by reducing the fatality rates significantly. However it also shows confirmations are likely coming this fall/winter.

Unfortunately coinciding with reports of vaccine effectiveness concerns beyond 6 months – bulk of vaccination in April – which puts the vaccine effectiveness in question for this Winter.

We do know with much certainty that natural immunization is more effective than vaccines – it would be a decent strategy to be healthy and have taken the vaccine and then to naturally expose oneself to covid and recover.
Knowing what we know now and seeing how things played out – we will see significant confirmations this winter much higher than last year – the positive news the fatality rate will likely be 70% lower – so we will likely see around 1% peak fatality rate. Unfortunately this will be a bigger number times this smaller number. I suspect we could see 2X the level of confirmation last year if we maintain the current trend and not change public building HVAC systems and/or social behaviors.
It would seem based on media that younger people are dying more than before – it has grown but not as much as you would think per the media. The morbid fact the pool of 85+ is lower so the that category has dropped from peak of 35% to 17%. The 0-24 has jumped from 0.14% to 0.4% – so 4X growth but very small numbers.

Deaths are still way lower so the denominator is impacting the percent calc.

Based on the above we can compute the estimated deaths by age for this winter and the odds. Overall deaths this winter SHOULD drop 100K less than last year (40% less) – which would produce 193K deaths (Nov-Mar) for the high estimates. However the chances of death needs to be kept in perspective – the odds of dying in a car as an occupant is 1 in 47,852 – so don’t get in a car if you think that risk is too great. We cannot lockdown society for these types of odds particularly for the youth.

We are still observing greater than normal deaths (~1-2K/wk beyond covid deaths) this is likely driven by our policy to covid which resulted in the lack of health services and/or social impacts.

Once again our policy response needs to be measured with the risk above and the risk to the policy. In hindsight our policy to isolate kids did them a disservice – we see here that the youth got more obese than they were already due to the quarantine. Changes in Body Mass Index Among Children and Adolescents During the COVID-19 Pandemic | Adolescent Medicine | JAMA | JAMA Network
“Youths gained more weight during the COVID-19 pandemic than before the pandemic (Table). The greatest change in the distance from the median BMI for age occurred among 5- through 11-year-olds with an increased BMI of 1.57, compared with 0.91 among 12- through 15-year-olds and 0.48 among 16- through 17-year-olds. Adjusting for height, this translates to a mean gain among 5- through 11-year-olds of 2.30 kg (95% CI, 2.24-2.36 kg) more during the pandemic than during the reference period, 2.31 kg (95% CI, 2.20-2.44 kg) more among 12- through 15-year-olds, and 1.03 kg (95% CI, 0.85-1.20 kg) more among 16- through 17-year-olds. Overweight or obesity increased among 5- through 11-year-olds from 36.2% to 45.7% during the pandemic, an absolute increase of 8.7% and relative increase of 23.8% compared with the reference period (Table). The absolute increase in overweight or obesity was 5.2% among 12- through 15-year-olds (relative increase, 13.4%) and 3.1% (relative increase, 8.3%) among 16- through 17-year-olds. Most of the increase among youths aged 5 through 11 years and 12 through 15 years was due to an increase in obesity.”
Obviously we cant afford this trend as much of the death is tied to obesity.
I talked to someone who was in China during the first SARS issue and they had a policy that all the youth had to be outside during the day and they did sports activity to pass the time. Perhaps we should think about this? China is certainly concerned about their youth – Three hours a week: Play time’s over for China’s young video gamers | Reuters
Look what the Tokyo Medical Association decided to do – New Corona: Tokyo Metropolitan Medical Association Recommends Ivermedictin Administration to Prevent Serious Diseases: Nikkei
“Haruo Ozaki, president of the Tokyo Metropolitan Medical Association, proposed the urgent use of the drug at a press conference on September 9, mainly with the aim of preventing the seriousness of home recuperators in order to respond to the spread of the new coronavirus. He stressed that antipar parasitic drugs such as ivermedictin should be administered to coronal infected people, as they have been shown to prevent serious diseases overseas.
In addition to ivermedine, the government has asked for the use of the steroid-based anti-inflammatory drug dexamethasone. Mr. Ozaki said, "[Both] have few side effects; I want the government to consider it so that it can be treated at the level of a family doctor."
Both ivermedine and dexamethasone are prescribed in Japan. However, it has not been approved as a treatment for corona.”
The US continues to lead in confirmation.

Healthy states do show up low in terms of confirmation and deaths e.g. Colorado

On a per capita view still no conclusive evidence to say vaccination reduces transmission