The most talked about is the “reinfection” I purposely did not want to discuss this yesterday as I wanted more numbers to work with but so many people are talking about it and sensationalizing the results. https://www.npr.org/sections/coronavirus-live-updates/2020/04/17/836747242/in-south-korea-a-growing-number-of-covid-19-patients-test-positive-after-recover
The key part of this article which is not being highlighted from multiple “news sources” – “Another possibility is that tests are picking up dead virus particles that are no longer infectious or transmissible. KCDC director-general Jeong Eun-kyeong said Friday that viruses collected from six relapse cases could not be cultivated in isolation, signifying that they are either dead or too small in number. But some relapsed patients may have living viruses that make them sick. As of Friday, at least 61 developed symptoms, albeit mild.” “KCDC has also mentioned errors in testing or sample collecting as potential causes.”
Even CNN noted in the middle of their article – cant grab you to read if they start off with the boring conclusion – https://www.cnn.com/2020/04/17/health/south-korea-coronavirus-retesting-positive-intl-hnk/ “In each of these cases, scientists tried to incubate the virus but weren’t able to — that told them there was no live virus present.
Like many countries, South Korea uses a reverse transcription polymerase chain reaction (RT-PCR) to test for the virus. The RT-PCR test works by finding evidence of a virus’s genetic information — or RNA — in a sample taken from the patient.
According to Kwon, these tests may still be picking up parts of the RNA even after the person has recovered because the tests are so sensitive.”
Just like vaccines which uses a weakened or kill form – this could be what we have here – and people do observe mild symptoms when given vaccine for the regular flu. The newness of the test and the mass testing effort done by S. Korea clearly leaves some room for test error to. In addition given these patients recovery – perhaps they were more brazen in their habits and repicked up the virus and the body was in the process of eliminating it – hence mild symptoms. The most controlled testing of re-infection still is the monkey study done in China – https://www.biorxiv.org/content/10.1101/2020.03.13.990226v1.full.pdf Where they conclude “In this study, our results indicated that the primary SARS-CoV-2 infection could protect from subsequent
exposures, which have the reference of prognosis of the disease and vital implications for vaccine design. Importantly, the unsuccessful rechallenge in NHP models suggested that the re-positivity from discharged patients could not be due to reinfection. It needs to consider more complicated issues to find out the causes”
There is a pessimistic potential for reinfection but to be fair and balance I think equally if not more there is optimism in that the “reinfections” are not what is claimed in the headlines.
Not the best source of news but it’s a worthy subject to consider the stress factor of poverty and eventually to THINK is there a better approaches perhaps for next time – https://gulfnews.com/amp/world/asia/india/the-human-cost-of-indias-coronavirus-lockdown-deaths-by-hunger-starvation-suicide-and-more-1.1586956637547?
Can we find the limiting factor in the healthcare supply chain and focus on minimizing that vs. locking the whole sectors…are there smarter ways – particularly “SMART”quarantine – perhaps have healthscreening for known issues that cause hospitalization find those and quarantine those – a way to phase back in?
US Poverty Death Rate
https://www.sciencedaily.com/releases/2011/06/110616193627.htm
The investigators found that approximately 245,000 deaths in the United States in the year 2000 were attributable to low levels of education, 176,000 to racial segregation, 162,000 to low social support, 133,000 to individual-level poverty, 119,000 to income inequality, and 39,000 to area-level poverty.
Overall, 4.5% of U.S. deaths were found to be attributable to poverty — midway between previous estimates of 6% and 2.3%. However the risks associated with both poverty and low education were higher for individuals aged 25 to 64 than for those 65 or older.
"Social causes can be linked to death as readily as can pathophysiological and behavioral causes," points out Dr. Galea, who is also Gelman Professor of Epidemiology. For example, the number of deaths the researchers calculated as attributable to low education (245,000) is comparable to the number caused by heart attacks (192,898), which was the leading cause of U.S. deaths in 2000. The number of deaths attributable to racial segregation (176,000) is comparable to the number from cerebrovascular disease (167,661), the third leading cause of death in 2000, and the number attributable to low social support (162,000) compares to deaths from lung cancer (155,521).
In 2000 31 million considered poverty – so death rate 0.8%. This is not an argument for free for all but a search for a “SMART” quarantine approach – perhaps there are not any but if you don’t question you will never know. S. Korea is worthwhile country to learn from – see below notes.
Positive news
Who would of thought Napolean Dynamite was on to something – https://arynews.tv/en/study-llama-blood-antibodies-coronavirus/ “New study reveals llama blood contains antibodies for combating coronavirus” “The antibodies, first used in HIV research, have proved effective against a viruses such as Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS) in the past.”
Breath analyzer test under a minute underdevelopment – https://m.jpost.com/health-science/diagnosing-the-coronavirus-in-under-a-minute-with-israeli-tech-625123/amp
Sweden approach looks to be way too early to conclude much – if anything S. Korea has the gold star – https://www.bloomberg.com/amp/news/articles/2020-04-19/sweden-says-controversial-covid-19-strategy-is-proving-effective?
Sweden should have lower numbers than many European country as their population density is lower – also testing per capita is lower. S. Korea on the other hand their approach to epidemic deserves great praise given how dense their population is and the amount of testing done per capita.

Weekend data always suspect – wishful thinking the downward gains are real

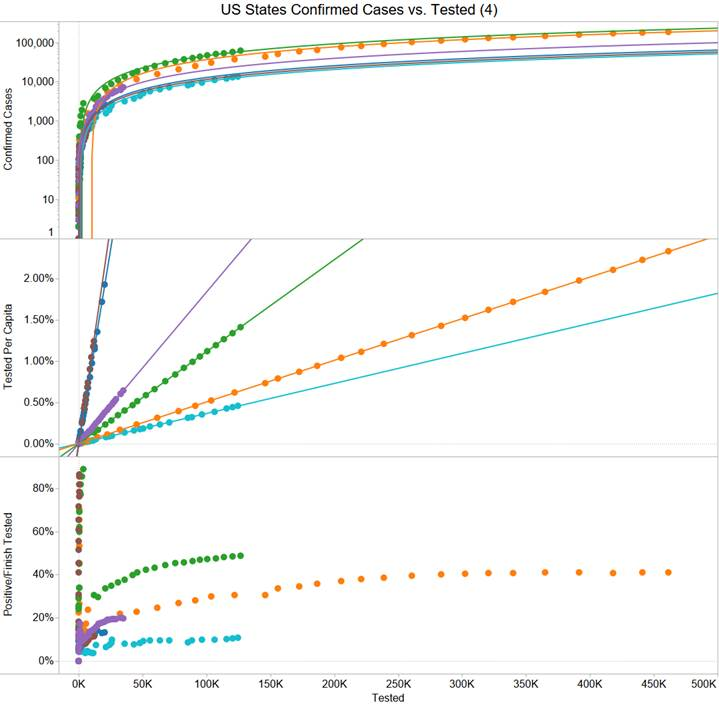
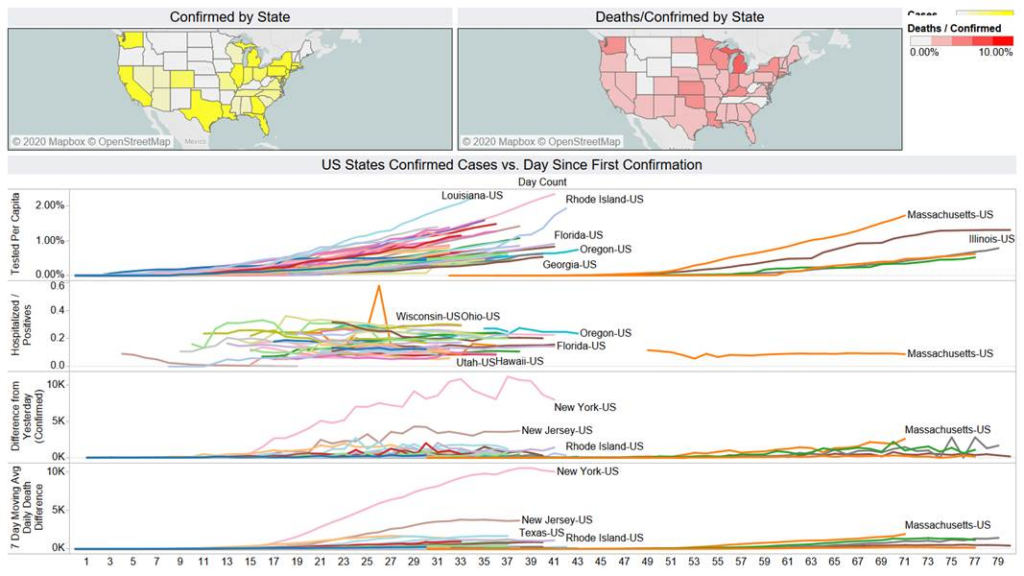
If you want some silver lining the positive/tested are flat lining for many states – so it could mean the method of testing is consistent – but overall no one is near NY level of 40%. Texas is at 10% and at 0.67% per capita tested now.

On a state basis NY has tested more than anyone in the world on a per capita bases. Worldwide testing data not consistent – but below chart gives a depiction on what is going on. France is very far behind in terms of testing (red line).

Lets hope the weekend lull is real – even Brazil looking to flatten out now. Sweden still looks to going up though.